Hip Pain: Causes, Symptoms, and Treatment Options
Hip pain can come from the joint itself, from surrounding tendons and bursae, or from the spine and pelvis. Identifying the true source makes all the difference in choosing the right treatment.
The hip is a ball-and-socket joint that bears the body's full weight during standing, walking, and climbing stairs. Pain can arise from the joint itself, the surrounding tendons and bursae, or from referred sources such as the lumbar spine.
What is Hip Pain?
True hip joint pain is typically felt in the groin and sometimes in the front of the thigh. Outer hip and buttock pain more often comes from the greater trochanteric region, gluteal tendons, or the sacroiliac joint.
This distinction matters because treating the wrong structure will not provide relief. A thorough clinical assessment, combined with targeted diagnostic injections when needed, identifies the true pain source.
Many people with hip pain can be treated effectively without surgery. Interventional procedures provide significant, durable relief for the most common hip pain conditions.

Symptoms of Hip Pain
Common symptoms include:
See a specialist if hip pain has lasted more than 4 weeks, is affecting your gait, or comes with significant stiffness or inability to weight-bear.
- Pain in the groin, outer hip, or buttock
- Stiffness when getting up from a chair or after lying down
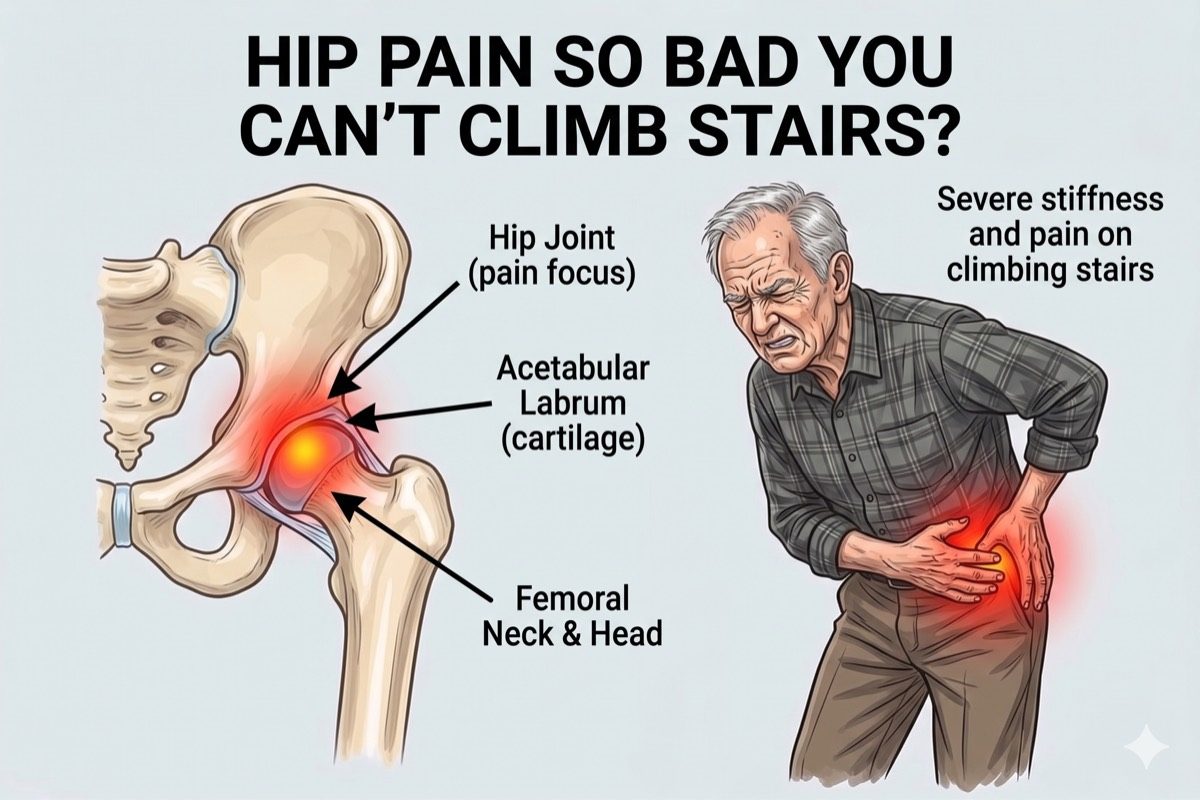
- Pain that worsens with walking, climbing stairs, or prolonged standing
- Referred pain into the thigh or knee
- Difficulty with hip rotation or putting on shoes and socks
- A limp or altered walking pattern to avoid pain
- Pain at night when lying on the affected side
What Causes Hip Pain?
The most common causes are:
Risk factors include excess body weight, leg length discrepancy, prior hip injury, high-impact sports, and age-related changes in the joint.
- Hip Osteoarthritis: Cartilage in the hip joint wears down progressively, causing groin pain, stiffness, and a reduced range of motion. It is the most common cause of true hip joint pain in adults over 50.
- Greater Trochanteric Pain Syndrome: Inflammation of the trochanteric bursa and gluteal tendons causes pain on the outer side of the hip, worse when lying on it or climbing stairs. It is often misdiagnosed as hip joint arthritis.
- Sacroiliac Joint Dysfunction: The joint connecting the spine to the pelvis becomes inflamed or unstable, causing pain in the lower back, buttock, and outer hip that can mimic hip joint disease.
- Meralgia Paresthetica: Compression of the lateral femoral cutaneous nerve at the groin causes burning, tingling, or numbness over the outer thigh. It is commonly caused by tight clothing, obesity, or prolonged sitting.
- Hip Labral Tear: A tear in the cartilage rim of the hip socket causes a deep groin ache, a clicking sensation, and pain with rotational movements.
Greater Trochanteric Pain Syndrome
Greater Trochanteric Pain Syndrome (GTPS) is one of the most common and frequently missed causes of hip-area pain. It involves inflammation or degeneration of the gluteal tendons and the bursa overlying the greater trochanter, the bony prominence on the outer side of the upper thigh.
It is often confused with hip osteoarthritis because both cause lateral hip pain in middle-aged and older adults. However, in GTPS the groin is not painful and hip rotation is usually preserved.
An ultrasound-guided trochanteric bursa injection is highly effective for this condition and can provide lasting relief, avoiding the need for surgery in the vast majority of cases.
How is Hip Pain Diagnosed?
Dr. Ashu Kumar Jain begins with a structured clinical examination to determine whether the pain is coming from inside the joint, from the surrounding soft tissues, or from the spine. This shapes which investigations are needed.
- Clinical examination including FABER, FADIR, and Trendelenburg tests to assess joint and tendon function
- X-rays (weight-bearing) to assess hip joint space and femoral head changes
- MRI for labral tears, tendon assessment, and bone marrow changes
- Ultrasound for real-time assessment of the trochanteric bursa and gluteal tendons
- Diagnostic hip joint or trochanteric bursa injection to confirm the primary pain source
Check If You Need This Treatment
I have persistent groin, outer hip, or buttock pain
My X-ray or MRI shows hip joint changes or tendon/bursa involvement
Pain has lasted more than 4 to 6 weeks
Pain limits my walking or daily activities
Conservative treatments haven’t fully helped
What we offer?
Our approach to treating hip pain
We use targeted, minimally invasive procedures that go directly to the source of the pain.
 Hip Joint Injection (intra-articular corticosteroid) for hip osteoarthritis and joint inflammation
Hip Joint Injection (intra-articular corticosteroid) for hip osteoarthritis and joint inflammation- Greater Trochanteric Bursa Injection for lateral hip pain and trochanteric pain syndrome
- Sacroiliac Joint Injection for SI joint-related buttock and hip pain
- Lateral Femoral Cutaneous Nerve Block for meralgia paresthetica and outer thigh pain
- Genicular Nerve Blocks of the Hip Joint followed by Cooled Radiofrequency Ablation for mild to moderate hip osteoarthritis or avascular necrosis of the femoral head
- Regenerative Therapy (PRP / Prolotherapy) for early osteoarthritis of the hip joint

Frequently asked questions
How do I know if my hip pain is from the joint or from the bursa?
True hip joint pain is usually felt in the groin and worsens with internal rotation of the hip. Trochanteric bursa pain is felt on the outer side of the hip and is tender to touch over the greater trochanter. A diagnostic injection into either structure can confirm the source when the clinical picture is unclear.
What is better for greater trochanteric bursitis: corticosteroid injection or PRP therapy?
For greater trochanteric bursitis with associated gluteal tendon involvement, PRP (platelet-rich plasma) therapy is the preferred option. Corticosteroid injections provide faster short-term relief but their benefit typically lasts only a few weeks, and repeated injections can weaken tendon tissue over time. PRP stimulates the body's own healing response in the tendon and bursa, producing more durable improvement. For purely inflammatory bursal flare-ups without significant tendon degeneration, a corticosteroid injection remains a reasonable first step. Your treatment choice is guided by the severity of tendon involvement seen on ultrasound or MRI.
What is meralgia paresthetica?
Meralgia paresthetica is compression of the lateral femoral cutaneous nerve as it passes under the inguinal ligament at the groin. It causes burning pain, numbness, or tingling over the outer thigh. It is common in people who are overweight, wear tight clothing, or sit for long periods. A targeted nerve block is very effective.
What interventional treatments are available for hip pain?
We offer image-guided hip joint injections for osteoarthritis, greater trochanteric bursa injections for lateral hip pain, sacroiliac joint injections for SI-related pain, and lateral femoral cutaneous nerve blocks for outer thigh numbness and burning. The right procedure is selected after a thorough diagnostic assessment.
Can hip pain be confused with back pain?
Yes, frequently. The lumbar spine and sacroiliac joint commonly refer pain into the buttock and hip region. Hip osteoarthritis can also refer pain to the knee, appearing to originate from the knee rather than the hip. This overlap makes a precise clinical assessment essential before any injection is done.
How long do hip injections last?
Hip joint corticosteroid injections typically provide relief for 6 to 12 weeks, though some patients experience longer-lasting benefit. Trochanteric bursa injections often produce more sustained results when combined with a rehabilitation programme. The duration depends on the severity of the underlying condition and individual response.
When should I see a specialist for hip pain?
See a pain specialist if your hip pain has lasted more than 4 weeks, is limiting your walking or sleep, or is not responding to rest and oral medication. Early intervention helps prevent the pain from becoming chronic and often avoids the need for surgical management.