Trigeminal Neuralgia, the Suicide Disease: Causes, Symptoms, and Treatment
Trigeminal neuralgia is also called the suicide disease because the pain is so severe that many patients have attempted suicide. With the right interventional treatment, significant and lasting relief is achievable.

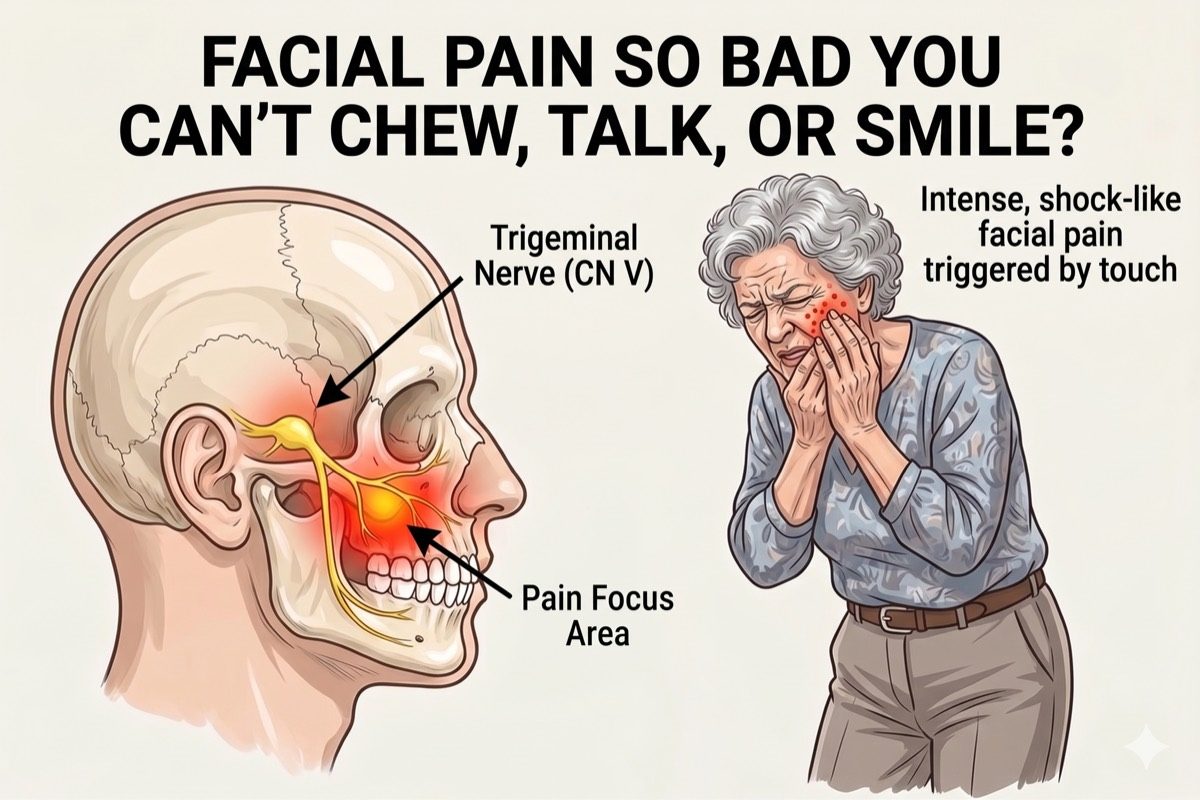
The trigeminal nerve is the fifth cranial nerve and the main sensory nerve of the face. When it malfunctions and fires abnormal pain signals, it causes sudden, severe bursts of facial pain that can be debilitating. Trigeminal neuralgia is widely known as the suicide disease because the intensity of the pain has driven many patients to attempt suicide, making prompt and effective treatment essential.
What is Trigeminal Neuralgia?
Trigeminal neuralgia causes sudden, severe, electric shock-like or stabbing pain on one side of the face. The pain is typically brief, lasting from a few seconds to two minutes, but can occur repeatedly throughout the day.
The trigeminal nerve has three branches: the ophthalmic branch (V1) supplying the forehead and eye, the maxillary branch (V2) supplying the cheek and upper jaw, and the mandibular branch (V3) supplying the lower jaw. Pain most often affects V2 and V3.
The condition is more common in people over 50 and affects women slightly more than men. Left untreated, episodes tend to become more frequent and more severe over time.

Symptoms of Trigeminal Neuralgia
Common symptoms include:
- Sudden, severe, electric shock-like or stabbing pain in the face
- Episodes lasting from a few seconds to about two minutes
- Pain consistently on one side of the face
- Triggering with light touch: eating, speaking, brushing teeth, a light breeze, or washing the face
- Pain-free periods between attacks in the classic type
- A constant aching background pain in the atypical type
- Episodes becoming more frequent and intense over time without treatment
See a specialist promptly if facial pain is interfering with eating, speaking, or daily life. Early treatment prevents episodes from escalating.
What Causes Trigeminal Neuralgia?
The most common causes are:
- Vascular Compression: A blood vessel pressing on the trigeminal nerve root as it exits the brainstem. This is the most common identifiable cause and disrupts normal nerve signalling.
- Multiple Sclerosis: Demyelination of the trigeminal nerve root by MS plaques can cause trigeminal neuralgia, typically in younger patients.
- Tumours: Rarely, a tumour near the nerve root compresses it, producing similar symptoms. MRI imaging rules this out in all new cases.
- Post-Traumatic or Post-Dental: Nerve injury following facial trauma or dental procedures can sensitise the trigeminal nerve and produce persistent pain.
- Post-Herpetic Neuralgia (PHN): A previous herpes zoster (shingles) infection affecting the trigeminal nerve can leave behind persistent nerve pain. PHN primarily involves the V1 (ophthalmic) division, causing burning pain in the forehead and around the eye.
In most cases, no identifiable structural cause is found on imaging. This is called Classical or Primary Trigeminal Neuralgia. The nerve fires abnormally without a clear underlying lesion, and effective treatment is still achievable in these cases.
Classic vs Atypical Trigeminal Neuralgia
Classic trigeminal neuralgia (Type 1) is purely episodic. There is no background pain between attacks, and episodes are sharply triggered by light stimulation. This type responds best to interventional treatment.
Atypical trigeminal neuralgia (Type 2) involves a constant aching or burning background pain in addition to episodic attacks. It is more difficult to treat and often requires a combination of medication and interventional procedures.
Correctly identifying the type guides the choice of treatment. A detailed pain history is the most important diagnostic step, and Dr. Ashu Kumar Jain will assess both types carefully before recommending a plan.
How is Trigeminal Neuralgia Diagnosed?
Diagnosis is primarily clinical, based on a detailed description of the pain. The character, distribution, and trigger pattern of the pain are highly specific and allow a confident diagnosis in most cases.
- Detailed clinical history focusing on pain character, triggers, duration, and distribution across facial branches
- MRI brain with dedicated trigeminal nerve protocol to identify vascular contact, MS lesions, or tumours
- Neurological examination to assess facial sensation and exclude other conditions
- Pain mapping to identify which branches (V1, V2, V3) are affected and guide procedure targeting
Check If You Need This Treatment
What we offer?
Our approach to treating trigeminal neuralgia
We use targeted, minimally invasive procedures that go directly to the source of the pain.
-
 Conventional Radiofrequency Ablation (RFA) of the Gasserian Ganglion delivering thermal energy at 60–70°C for 80 seconds, providing pain relief for 5–10 years
Conventional Radiofrequency Ablation (RFA) of the Gasserian Ganglion delivering thermal energy at 60–70°C for 80 seconds, providing pain relief for 5–10 years
-
In-house MRI brain with trigeminal protocol to rule out structural causes before any procedure
-
Peripheral Trigeminal Nerve Block for temporary relief from acute facial pain episodes
Frequently asked questions
Why is Conventional RFA the preferred treatment for Trigeminal Neuralgia?
Conventional RFA is the most effective interventional treatment for trigeminal neuralgia. It works by delivering thermal energy at 60–70°C for 80 seconds directly to the Gasserian ganglion, disrupting the pain-carrying fibres of the trigeminal nerve. This provides durable pain relief lasting 5–10 years for most patients, allowing a return to normal daily life free from debilitating facial pain episodes.
What is the duration of pain relief after conventional RFA?
Most patients experience pain relief for 5 to 10 years after a successful conventional RFA procedure. The duration can vary depending on the individual, but for many, the improvement is long-lasting and allows a return to normal activities without frequent pain episodes.
Is the pain relief after conventional RFA permanent or can it reoccur?
Pain relief after conventional RFA is long-lasting for most patients, but it is not always permanent. Pain can reoccur after 5 to 10 years as the nerve may regenerate or become sensitised again. If pain returns, further treatment options are available.
Can we repeat conventional RFA if pain reoccurs?
Yes, conventional RFA can be safely repeated if pain returns. Even if it comes back as early as 3 months after the first procedure, many patients who experience a recurrence of trigeminal neuralgia undergo repeat conventional RFA with good results and minimal risk.
Can conventional RFA of the trigeminal ganglion cause paralysis or stroke?
No, conventional RFA of the trigeminal ganglion does not cause paralysis or stroke. The procedure is highly targeted and performed with precision to avoid injury to surrounding structures. Complications are extremely rare when performed by an experienced specialist.
Why is trigeminal neuralgia pain so severe?
The trigeminal nerve has one of the highest densities of sensory fibres of any nerve in the body. When it fires abnormally, the brain receives an overwhelming pain signal from the face. The sudden, uncontrolled nature of these signals is what makes the pain so intense and distressing. Effective treatment directly targets and calms this abnormal nerve activity.
Is trigeminal neuralgia a dental problem?
No. Trigeminal neuralgia is a neurological condition, not a dental one. Many patients are initially misdiagnosed and undergo unnecessary dental procedures before the correct diagnosis is made. The pain may feel like a severe toothache but a careful history, particularly the trigger pattern and episodic nature, points clearly to a nerve origin.
What is the difference between a nerve block and Conventional RFA for trigeminal neuralgia?
A peripheral trigeminal nerve block uses local anaesthetic to temporarily numb the nerve, providing short-lived relief that lasts only weeks to months. It is not a recommended long-term solution. Conventional RFA at the Gasserian ganglion, by contrast, delivers targeted thermal energy at 60–70°C for 80 seconds to ablate the pain-carrying fibres of the nerve. This gives lasting relief of 5–10 years and is the treatment of choice for trigeminal neuralgia.
Will medication alone control trigeminal neuralgia?
Carbamazepine is the first-line medication and controls attacks in many patients initially. However, over time the medication may lose effectiveness, require dose increases that cause side effects, or fail to provide adequate control. Interventional procedures are then the most appropriate next step and are very effective, especially for classic trigeminal neuralgia.
Is surgery necessary for trigeminal neuralgia?
Microvascular decompression surgery is an option for suitable candidates with classical neuralgia and confirmed vascular compression, but it carries surgical risks. Conventional RFA offers an effective, minimally invasive alternative that provides 5–10 years of pain relief and is preferred for patients who are not good surgical candidates or who want to avoid open surgery.
When should I see a pain specialist for facial pain?
See a pain specialist if you have sudden, severe, episodic facial pain that is triggered by light touch or eating, if medication is not providing adequate control, or if side effects from medication are affecting your daily life. Early specialist assessment ensures the correct diagnosis and prevents unnecessary treatments.
Any concern?