Knee Pain: Causes, Symptoms, and Treatment Options
Knee pain is one of the most common musculoskeletal complaints, affecting people of all ages. Most causes are treatable with targeted interventional procedures that provide lasting relief without surgery.
The knee is a complex weight-bearing joint that absorbs significant stress with every step. Pain can arise from the joint cartilage, surrounding tendons, bursae, or the nerves supplying the knee.
What is Knee Pain?
Knee pain can be felt at the front, side, or back of the knee, and it can stem from structures inside the joint or outside it. It may come on suddenly after an injury, or develop gradually from wear and tear over time.
Osteoarthritis is the most common cause in adults over 50. In younger people, conditions like patellofemoral pain syndrome and meniscal tears are more frequent.
Many patients with knee pain can be treated effectively without surgery. Identifying the exact source of pain is the key to selecting the right procedure.

Symptoms of Knee Pain
Common symptoms include:
- Pain at the front, inner, outer, or back of the knee
- Swelling or warmth around the joint
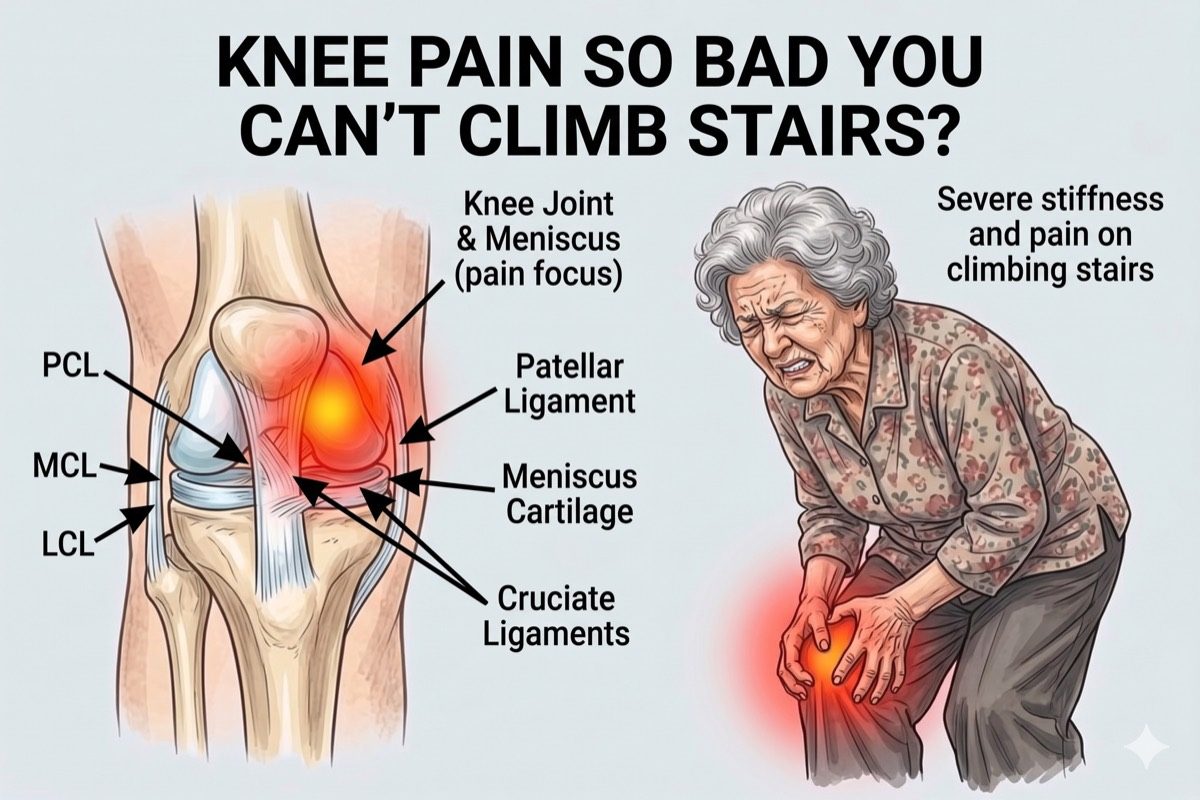
- Stiffness, especially in the morning or after sitting for long periods
- A grinding, clicking, or locking sensation during movement
- Pain that worsens when climbing or descending stairs
- Difficulty fully bending or straightening the knee
- A feeling of the knee giving way or being unstable
See a specialist if knee pain has lasted more than 4 weeks, is limiting your mobility, or comes with significant swelling or instability.
What Causes Knee Pain?
The most common causes are:
- Knee Osteoarthritis: Cartilage in the joint wears down gradually, causing bone-on-bone friction, pain, swelling, and progressive stiffness. It is the most common cause of knee pain in adults over 50.
- Patellofemoral Pain Syndrome: Pain behind or around the kneecap caused by abnormal tracking of the patella during movement. Common in younger, active individuals.
- Meniscal Tear: A tear in the cartilage pad between the thigh and shin bones causes pain, swelling, and a catching or locking sensation in the knee.
- Pes Anserine Bursitis: Inflammation of the bursa on the inner side of the knee just below the joint, commonly causing medial knee pain in overweight adults and runners.
- Referred Pain from the Hip or Lumbar Spine: Hip osteoarthritis and lumbar nerve root irritation frequently refer pain to the knee, making accurate diagnosis essential.
Risk factors include excess body weight, prior knee injury, repetitive kneeling or squatting, age, and a sedentary lifestyle.
Knee Osteoarthritis
Knee osteoarthritis is graded from 1 (mild) to 4 (severe) based on X-ray findings. Even grade 3 or 4 osteoarthritis can be managed effectively with interventional procedures that reduce pain and improve function, delaying or avoiding the need for knee replacement surgery.
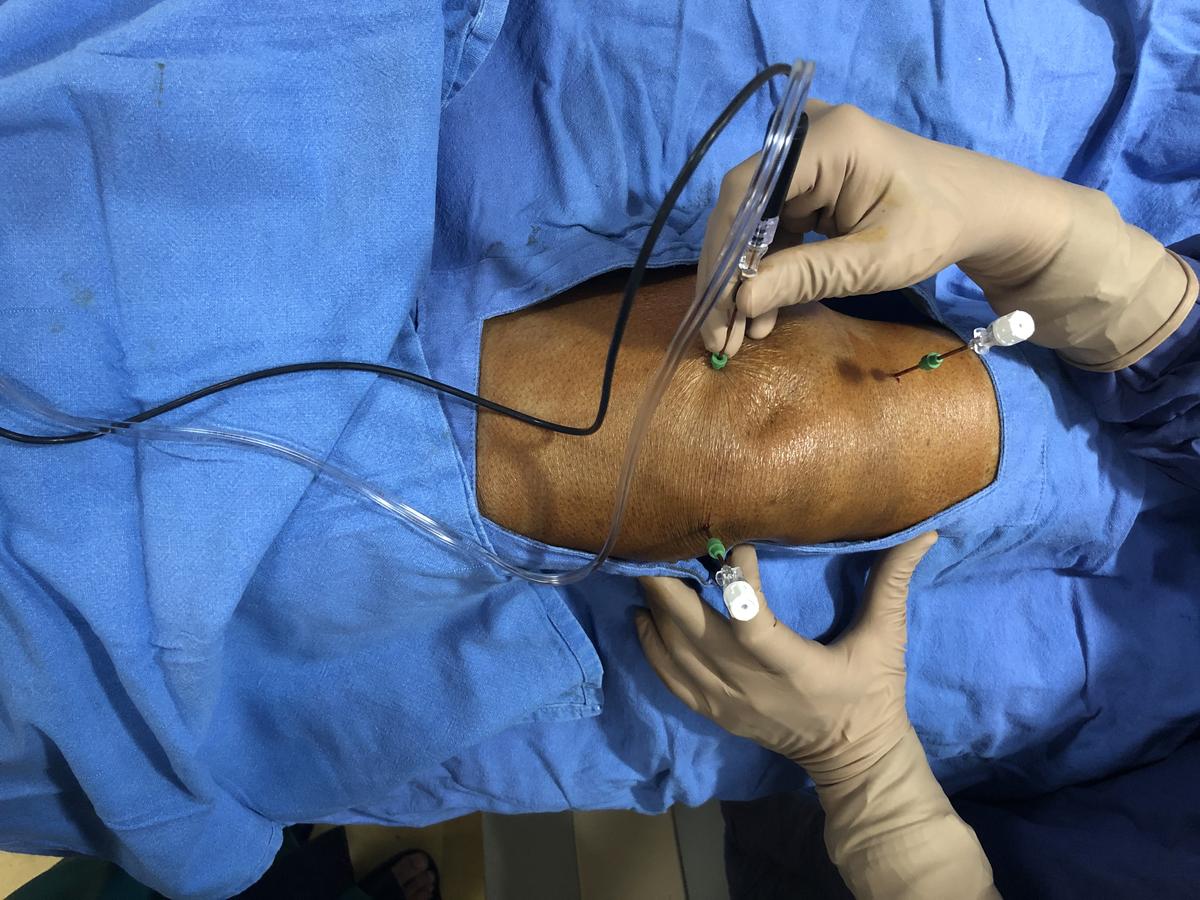
The genicular nerves are the small sensory nerves that supply pain signals from the knee joint. Blocking or ablating these nerves is one of the most effective interventional techniques for knee osteoarthritis and provides relief without altering the joint itself.
Genicular Radiofrequency Ablation (RFA) can provide 9 to 18 months of significant pain relief, and the procedure can be repeated as needed.
How is Knee Pain Diagnosed?
Diagnosis begins with a clinical examination and a review of symptoms. Dr. Ashu Kumar Jain assesses gait, joint line tenderness, range of motion, and stability before recommending imaging.
- Clinical examination including joint line palpation, McMurray test, and patellar assessment
- X-rays (weight-bearing) to assess joint space narrowing and bone spurs
- MRI for soft tissue assessment including menisci, cartilage, and tendons
- Ultrasound for real-time assessment of bursae and tendon integrity
- Diagnostic genicular nerve block to confirm suitability for RFA
Check If You Need This Treatment
What we offer?
Our approach to treating knee pain
We use targeted, minimally invasive procedures that go directly to the source of the pain.
-
 Genicular Nerve Block for rapid diagnosis and immediate relief from knee osteoarthritis pain
Genicular Nerve Block for rapid diagnosis and immediate relief from knee osteoarthritis pain
-
Genicular Radiofrequency Ablation (RFA) for long-term pain relief lasting 9 to 18 months
-
Intra-articular Corticosteroid Injection to reduce joint inflammation and swelling
-
Hyaluronic Acid (Viscosupplementation) Injection to improve joint lubrication and reduce pain
-
Regenerative Therapies including PRP (Platelet-Rich Plasma) and stem cell therapy (bone marrow or adipose tissue derived, and mesenchymal stem cells) for grade 1 to 3 knee osteoarthritis
Frequently asked questions
What is genicular nerve RFA and how does it help knee pain?
Genicular RFA uses radiofrequency energy to disrupt the small sensory nerves that carry pain signals from the knee joint. It does not affect the joint structure itself. The procedure typically provides 9 to 18 months of significant pain relief and can be repeated. It is most effective for knee osteoarthritis.
Am I a candidate for genicular RFA?
Good candidates are patients with moderate to severe knee osteoarthritis who have had at least 50% temporary pain relief from a diagnostic genicular nerve block. A detailed clinical assessment will determine suitability. Even patients with grade 3 or 4 arthritis who are not ready or suitable for surgery often benefit significantly.
What is the difference between a cortisone injection and hyaluronic acid injection?
Cortisone (corticosteroid) injections reduce inflammation quickly and typically provide relief for 6 to 12 weeks. Hyaluronic acid injections lubricate and cushion the joint, with a more gradual onset but potentially longer-lasting effect. They work differently and may be recommended at different stages of osteoarthritis.
Can knee pain be referred from the hip or back?
Yes. Hip osteoarthritis commonly causes groin pain that the patient feels in the knee. Lumbar nerve root irritation at L3 or L4 can also refer pain into the knee. This is why a full assessment of the hip and lumbar spine is always part of the evaluation before treating knee pain.
Will I need a knee replacement?
Not necessarily. Many patients with even advanced knee osteoarthritis achieve good pain control and quality of life with interventional procedures, avoiding or significantly delaying the need for knee replacement. Surgery is a last resort when pain is severe, function is markedly impaired, and all other options have been exhausted.
What is the role of regenerative therapies in knee osteoarthritis?
Regenerative therapies such as PRP (Platelet-Rich Plasma) and stem cell therapy play a useful role in knee osteoarthritis up to grade 3. They promote tissue repair and reduce joint inflammation. In grade 4 osteoarthritis, where cartilage loss is severe, regenerative therapies have no meaningful role.
Which is better: stem cell therapy or PRP therapy for knee pain?
Both are comparable in effectiveness for knee osteoarthritis. Neither has been shown to be clearly superior to the other. The choice depends on availability, patient preference, and clinical assessment.
How many sessions of stem cell therapy or PRP are needed for knee pain?
Stem cell therapy is given as a single session. PRP therapy requires 3 to 5 sessions, administered at four-week intervals.
What is the success rate of PRP therapy for knee pain?
The success rate is approximately 70%. Some patients experience a temporary increase in pain during the first or second session. This can usually be managed with a simple analgesic such as paracetamol.
Can I take anti-inflammatory medications while undergoing PRP therapy?
No. Steroids and anti-inflammatory medications (NSAIDs) must be stopped at least four weeks before starting PRP therapy. Taking these medications during treatment interferes with platelet activity and can cause the therapy to fail.
Can I have a blind PRP injection without imaging guidance?
No. PRP must be injected under ultrasound guidance, precisely at the site of tendinitis or muscle tear. A blind injection without imaging will not deliver the platelets to the correct location and will produce no benefit.
Do collagen supplements help in grade 4 knee osteoarthritis?
No. Collagen capsules, tablets, or sachets have no proven role in grade 4 knee osteoarthritis. At this stage of cartilage loss, supplemental collagen cannot reverse or meaningfully modify the condition.
What is the difference between osteoarthritis and rheumatoid arthritis of the knee?
Osteoarthritis is degenerative arthritis related to age and wear, where cartilage gradually breaks down over time. Rheumatoid arthritis is an inflammatory autoimmune condition in which the immune system attacks the joint lining, causing inflammation, pain, and joint damage. The two conditions have different causes and require different treatments.
Any concern?