Mid Back Pain: Causes, Symptoms, and Treatment Options
Mid back pain in the thoracic spine is often overlooked because it is less common than neck or lower back pain. But when it strikes, it can be severe and limiting. The right diagnosis points directly to the right treatment.
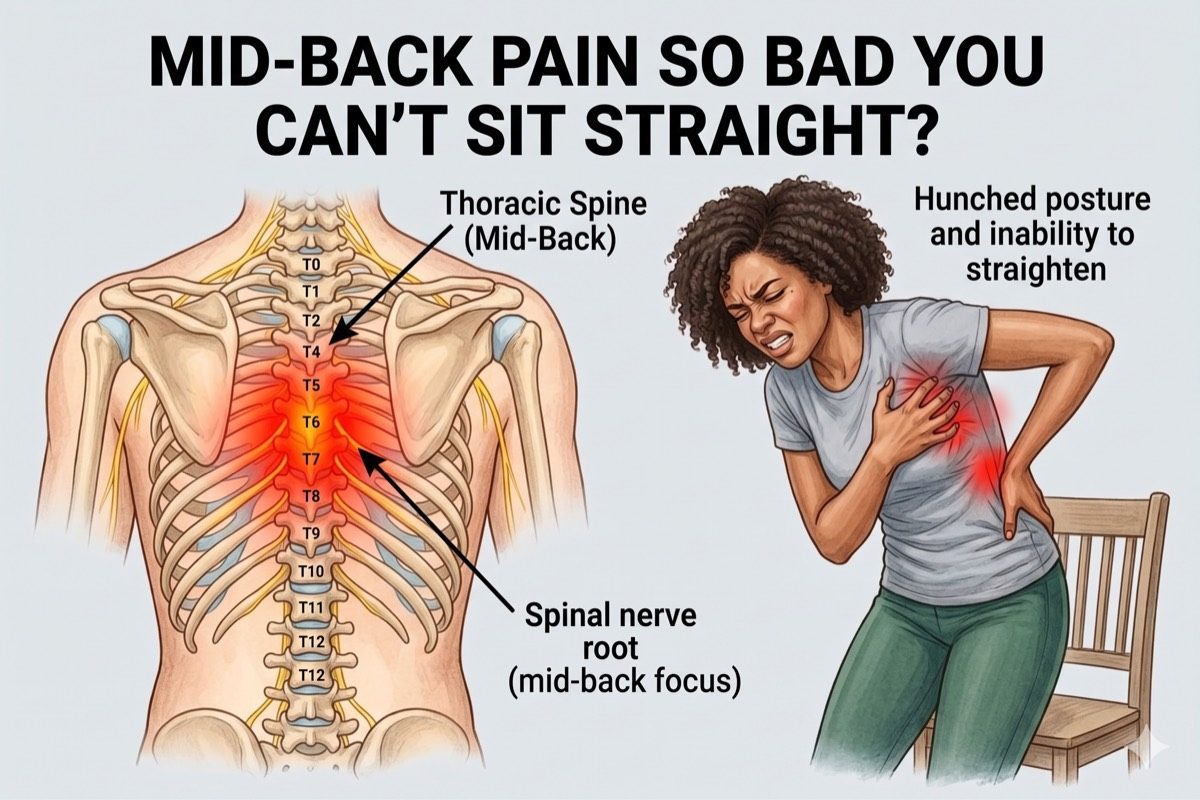
The thoracic spine runs from the base of the neck to the bottom of the rib cage, comprising twelve vertebrae (T1 to T12). Each vertebra connects to a pair of ribs, forming a sturdy but sometimes painful cage of joints.
What is Mid Back Pain?
Mid back pain refers to pain felt between the shoulder blades or anywhere along the thoracic spine. It may be dull and constant, or sharp and worsened by specific movements such as deep breathing, rotation, or bending.
Because the thoracic spine is stabilised by the ribcage, it moves less than the cervical or lumbar spine and is less prone to disc herniation. However, the facet joints between vertebrae and the joints where ribs meet the thoracic spine (costovertebral joints) are frequent sources of pain that often go undiagnosed.
Mid back pain can also be referred from internal organs, including the kidneys, gallbladder, and lungs. A thorough assessment rules out these sources before targeting spinal structures.

Symptoms of Mid Back Pain
Common symptoms include:
- Pain between or below the shoulder blades on one or both sides
- Pain that worsens with twisting, bending, or extending the spine
- Pain that increases with deep breathing, coughing, or sneezing
- Tenderness along the spine or at the rib junction when pressed
- Radiating pain around the rib cage following an intercostal nerve distribution
- Stiffness after prolonged sitting or on waking in the morning
- In severe cases, weakness, numbness, or altered sensation in the torso or legs
See a specialist promptly if mid back pain is accompanied by weakness in the legs, bowel or bladder changes, or pain after a fall or trauma, as these can indicate serious spinal pathology.
What Causes Mid Back Pain?
The most common causes are:
- Thoracic Facet Joint Arthropathy: Wear and tear of the facet joints between thoracic vertebrae causes paraspinal pain that worsens with extension and rotation. It is the most common interventionally treatable cause of mid back pain.
- Ankylosing Spondylitis: In younger patients, thoracic facet joint pain is frequently caused by ankylosing spondylitis, an inflammatory disease affecting the facet and sacroiliac joints of the spine. Unlike degenerative arthropathy, it is immune-mediated and typically presents with morning stiffness improving with activity. Early recognition is important as it requires specific medical management alongside interventional pain treatment.
- Costovertebral Joint Dysfunction: Each rib attaches to the thoracic spine at two small joints. Inflammation or degeneration of these joints causes unilateral mid back pain that typically worsens with deep breathing and lateral movements.
- Thoracic Disc Herniation: Less common than lumbar disc herniation but can cause nerve root compression producing sharp radiating pain around the chest wall (intercostal neuralgia) or, in severe cases, spinal cord compression.
- Intercostal Neuralgia: Irritation or damage to an intercostal nerve causes burning or sharp pain that wraps around the chest from back to front. Common causes include post-herpetic neuralgia (after shingles) and post-thoracotomy pain, which is persistent pain following chest surgery where intercostal nerves are stretched or damaged during the procedure.
- Osteoporotic or Metastatic Vertebral Fractures: Compression fractures in the thoracic vertebrae from osteoporosis or bone metastases cause acute, severe mid back pain, often occurring with minimal or no trauma.
Risk factors include poor posture, sedentary work, prior thoracic surgery, osteoporosis, and age-related degenerative changes.
Thoracic Facet vs Costovertebral Joint Pain
These two conditions are the most common interventionally treatable causes of mid back pain and are frequently confused with each other, as both produce paraspinal and lateral thoracic pain.
Thoracic facet joint pain is typically felt close to the midline, worsens with extension and rotation, and is reproduced by pressing on the paraspinal muscles adjacent to the involved levels. A thoracic medial branch block precisely diagnoses and treats this.
Costovertebral joint pain is more lateral, often felt at the rib angles, and characteristically worsens with deep breathing or coughing. This is because the rib-vertebra joint is stressed whenever the ribcage expands. A targeted costovertebral joint injection confirms and treats this source.
Correctly distinguishing these two conditions ensures the injection is placed in exactly the right structure, maximising benefit.
How is Mid Back Pain Diagnosed?
Diagnosis begins with a detailed clinical history and physical examination. Dr. Ashu Kumar Jain assesses spinal movement, palpates specific joint levels, and checks for neurological signs before recommending imaging.
- Clinical examination assessing spinal movement, paraspinal tenderness, and rib cage expansion
- X-rays to assess vertebral alignment, disc height, and any fractures or structural changes
- MRI for disc, nerve root, and spinal cord assessment, and to exclude referred sources
- CT scan for detailed bony anatomy when vertebral fracture or instrumented fusion is relevant
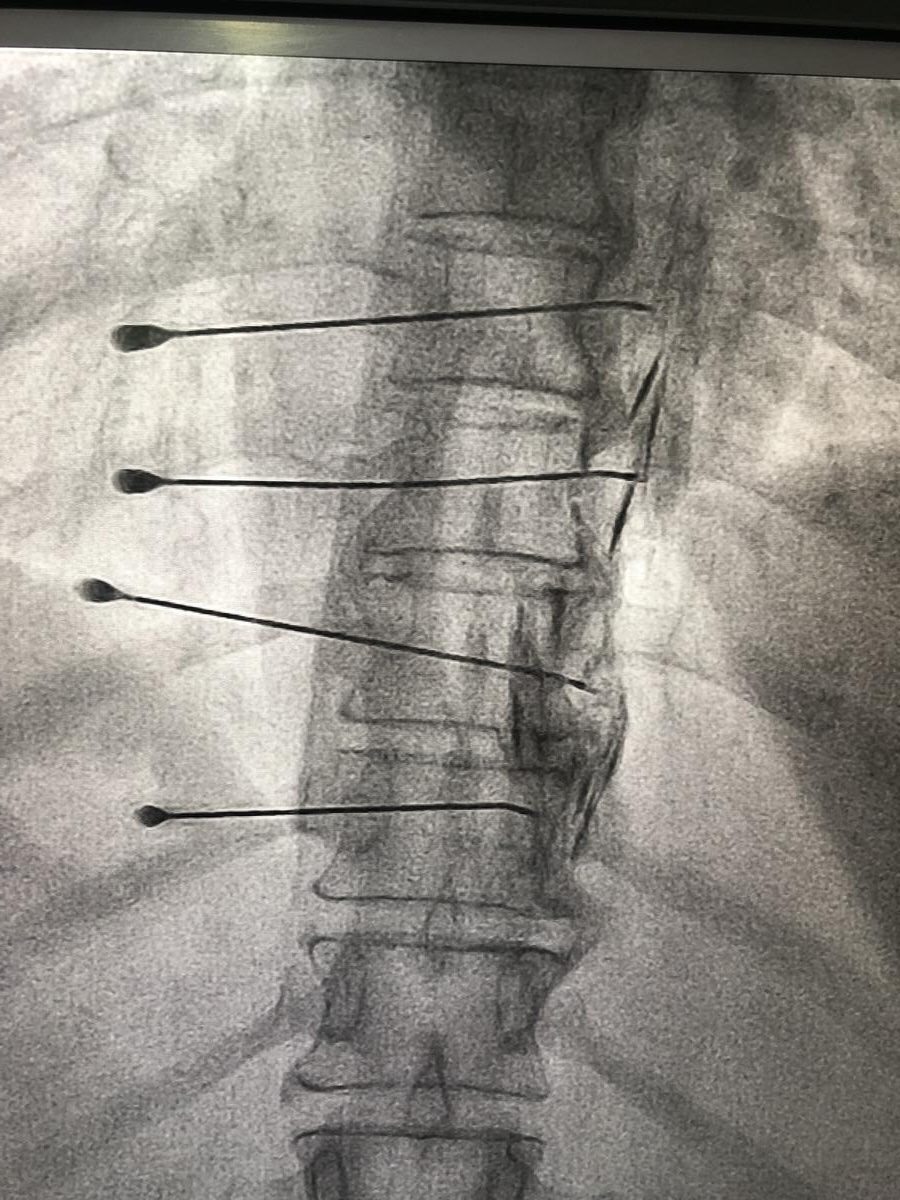
- Diagnostic medial branch block or costovertebral joint injection to confirm the pain source and guide definitive treatment
Check If You Need This Treatment
What we offer?
Our approach to treating mid back pain
We use targeted, minimally invasive procedures that go directly to the source of the pain.
-
 Thoracic Medial Branch Block to diagnose and provide immediate relief from thoracic facet joint pain
Thoracic Medial Branch Block to diagnose and provide immediate relief from thoracic facet joint pain
-
Thoracic Facet Cooled Radiofrequency Ablation (CRFA) for long-term relief from facet arthropathy lasting 9 to 18 months
-
Costovertebral Joint Injection targeting the rib-vertebra junction for lateral mid back and rib pain
-
Intercostal Nerve RFA / Neurolysis for thoracic nerve root pain, post-herpetic neuralgia, and rib cage pain
-
Thoracic Epidural Steroid Injection for disc-related nerve compression and thoracic radiculopathy
-
Thoracic Epidural Injection / DRG (Dorsal Nerve Root Ganglion) Ablation for acute herpesvirus infection and persistent intercostal nerve pain
Frequently asked questions
Why does my mid back pain worsen when I breathe deeply?
Deep breathing expands the ribcage, which stresses the costovertebral joints where the ribs attach to the thoracic vertebrae. Pain that specifically worsens with breathing suggests costovertebral joint dysfunction or intercostal nerve irritation as the likely source. A targeted injection into the costovertebral joint or intercostal nerve block is often highly effective for this type of pain.
Can mid back pain be caused by organ problems, not just the spine?
Yes. The kidneys, gallbladder, stomach, pancreas, and lungs can all refer pain to the thoracic back. This referred pain is an important consideration and is assessed during clinical evaluation. Red flags such as fever, weight loss, night sweats, or blood in the urine are investigated before any spinal intervention is carried out.
What is a thoracic medial branch block?
The medial branches are small nerves that carry pain signals from the thoracic facet joints. A medial branch block places a small amount of local anaesthetic on these nerves under image guidance. It serves two purposes: it immediately confirms whether the facet joints are the pain source, and it provides short-term relief. If it works well, a thoracic facet RFA can be performed for much longer-lasting relief.
Is mid back pain from shingles treatable?
Post-herpetic neuralgia (persistent pain after shingles) commonly affects the thoracic dermatomes, producing burning pain that wraps around the chest wall. An intercostal nerve block or thoracic epidural injection can provide significant relief during the acute phase of herpesvirus infection. For persistent post-herpetic neuralgia, Thoracic Dorsal Nerve Root Ganglion RFA or Intercostal Nerve RFA is a highly effective option that dramatically improves quality of life.
Can a vertebral compression fracture in the thoracic spine be treated?
Yes. Vertebroplasty or kyphoplasty can be performed to stabilise a painful thoracic compression fracture, whether from osteoporosis or bone metastases. Bone cement is injected into the collapsed vertebra, reducing pain rapidly, often within 24 to 48 hours. This significantly improves mobility and quality of life.
When should I see a specialist for mid back pain?
See a pain specialist if your mid back pain has lasted more than 4 weeks, is not responding to rest and physiotherapy, or is associated with radiating pain around the chest. Immediate attention is needed if there is any weakness in the legs, numbness in the abdomen or lower body, or difficulty with bladder or bowel control, as these may indicate spinal cord involvement.
Any concern?